

“Underuse is evidence by the fact that many scientifically sound practices are not used as often they should be, For example, biannual mammography screening in woman ages 40 to 69 has been proven beneficial and yet is performed less than 75 percent of the time.” This is the categorization of:
- A . Defects
- B . La of professionalism in Medical field
- C . La of care
- D . Healthcare practice
__________ is a term applied when the proper clinical car process is not executed appropriately, such as giving the wrong drug to a patient or incorrectly administering the correct drug.
- A . Underuse
- B . Overuse
- C . Misuse
- D . Illegal use
Crossing the Quality Chasm provided a blueprint for the future that classified and unified the components of quality through six aims for improvement, chain of effects, and simple rules for redesign of healthcare. The six aims for improvement, viewed also six dimensions of quality.
Which of the following is NOT out of those dimensions?
- A . Safe
- B . Care centered
- C . Efficient
- D . Effective
______________ can be measured by how well evidence-based practices are followed, such as the percentage of time diabetic patients receive all recommended care at each doctor visit, the percentage of hospital-acquired infections, or the percentage of patients who develop pressure ulcers (bed sores) while in the nursing home.
- A . Safe care
- B . Equitable care
- C . Effective care
- D . Timely care
Today’s patients’ perception of the quality of our healthcare system is not favourable. In healthcare, qualityis household word that evokes great emotion, including:
- A . Frustration and despair, exhibited by patients who experience healthcare services firsthand or family members who observe the care of their loved ones
- B . Anxiety over the ever-increasing costs and complexities of care
- C . Patient centered measures
- D . Timely care that may be experienced in terms of performance of services
There is a story of an intensive care unit (ICU) at Dominican Hospital in Santa Cruz Country, California. Dominican, a 379-bed community hospital, is part of the 41-hospital Catholic Healthcare West system. “We used to replace ventilator circuit for incubated patients daily because we thought this helped to prevent pneumonia,” explained Lee Vanderpool, vice president. “”But the evidence shows that the more you interfere with that device, the more often you risk introducing infection. It turns out it is often better to leave it alone until it begins to become cloudy, or ‘gunky,’ as the no clinicians say.”
The hospital staff learned an important lesson from this experience that:
- A . Evidence is more powerful than intuition
- B . Intuition is more powerful than evidence
- C . Efforts improve mortality rate
- D . Introduction f a new protocol, or any new idea, involves education
A number of attributes can characterize the quality of healthcare services. As, there are different groups involved in healthcare, such as physicians, patients and health insurers, tend to attach different levels of importance to particular attributes and as a result define quality care differently.
Which of the following is/are NOT out of those attributes?
- A . Technical performance
- B . Responsiveness to patient preferences
- C . Excess staff
- D . Amenities
Quality and technical performance refers to how well current scientific medical knowledge and technology are applied in a given situation.
It is usually assessed in terms of:
- A . Timeliness and accuracy of the diagnosis
- B . Appropriateness of therapy and other medical interventions are performed
- C . The quality of interpersonal relationships
- D . Both A & B
The quality of amenities of care refers to the characteristics of the setting in which the encounter between patient and clinician takes place, such as:
- A . Comfort
- B . Comfort, care and access
- C . Comfort, convenience and privacy
- D . Responsive to patient preferences
Amenities may cover areas as mentioned below EXCEPT:
- A . Ample and convenient parking
- B . Good directional signs
- C . Comfortable waiting rooms
- D . Vast and facilitated food providing area
_________________ refers to the “degree to which individuals and groups are able to obtain needed services.”
- A . Responsiveness to patient preferences
- B . Amenities
- C . Equity
- D . Access
In earlier formulations, responsiveness to patients’ preferences was just one of the factors seen as determining the quality of patient clinician interpersonal relationship. But, now it is translated into many factors.
Which of the following is out of such factors?
- A . Respect for patients’ values
- B . Respect for patients’ preferences
- C . Respect for patients’ expressed needs
- D . Respect for Respect for patient’s convenience
Efficiency refers how well resources are used in achieving a given result. Efficiency whenever the resources used to produce a given output are _____________.
- A . Reduces, reduced
- B . Increases, increased
- C . Improves, reduced
- D . It is truly situation dependent
In general, as the amounts spent on providing services for a particular condition grow, diminishing returns set in meaning that each unit of expenditure yield ever-smaller benefits until a point where ________________.
- A . No additional benefits accrue from adding more care
- B . Additional benefits are too small to justify the added costs
- C . There is displacement of more useful care
- D . perfection is within the reach of all individuals
“Quality is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”
This is the definition of Quality care often quoted by:
- A . IOM
- B . IHI
- C . HQCB
- D . OCHP
“Likelihood of desired health outcomes” corresponds to clinicians’ view that, with respect to outcomes, there are only probabilities, not certainties, owing to factors-such as patients’ genetically determined physiological reliance-that influence:
- A . The primary concerns of patients
- B . Outcomes of care and yet are beyond clinicians’ control
- C . Outcomes of care and now are within clinicians’ control
- D . High cost interventions
In fact, because patients’ satisfaction is so influenced by __________________ rather than to the more indiscernible technical ones-health maintenance organizations, hospitals and other health care delivery organizations have come to view the quality of nontechnical aspects of care as crucial to attractions and retaining patients.
- A . Their reactions to interpersonal and amenity aspect of care
- B . Patients recognize that they do not possess the wherewithal to evaluate all technical elements of care
- C . Every patient has definite preference in every clinical situation
- D . Their likelihood of desires outcomes
Payers are more likely to embrace the optimization definition of care which can put them at odds with:
- A . Clinicians
- B . Health administrators
- C . Physicians
- D . Both A & B
The manager’s perspective on quality differs markedly from that of clinicians and patients on:
- A . Efficiency, effectiveness and access
- B . Efficiency, cost effectiveness and equity
- C . Responsiveness to patient preferences
- D . Equity, access and technical performance
Strong disagreement do arise, among the five parties’ definitions (i.e. the clinician’s, the patient’s the payers, the manager’s and the society’s), even outside the realm of cost effectiveness.
Conflicts typically arise when:
- A . Practitioners who are highly skilled in trauma and other emergency care
- B . Each group emphasizes a particular aspect of care
- C . One party holds that a particular practitioner or clinic is a high quality provider by virtue of having high ratings on single aspect of care
- D . The facility receives top marks from a team of expert clinicians whose primary focus is on technical performance
All the evaluations of quality of care can be classified in terms of one three aspects of care giving they measure.
Which of the following is/are NOT out of these measures?
- A . Structure
- B . Process
- C . Output
- D . Cutbas
When quality is measured in terms of structure the focus is on the relatively static characteristics of the individuals who provide care and of the settings where the care is delivered. These characteristics include ____________ of professionals who provide care and the adequacy of the facility’s equipment, and overall organization.
- A . Education
- B . Training
- C . Certification
- D . A, B and C
Licensing and accrediting bodies have relied heavily on structural measures of quality not only because the measures are relatively stable and thus easier to capture but:
- A . They reliably indentify providers who are cheap
- B . They reliably identify providers who demonstrably la means to deliver high quality care
- C . They can never la the means to deliver high quality care
- D . They reliably identify physicians
Ordering the correct diagnostic procedure for a patient is a measure of _________. When evaluating the process of care, however, appropriateness is only half the story. The other half is in how well and how promptly (i.e. skill-fully) the procedure was carried out.
- A . Consciousness
- B . Appropriateness
- C . Care assessment
- D . Equity
Because of the goals of care can be defined broadly, outcome measures have come to include the costs of care as well as patients’ satisfaction with care.
In formulations that stress the technical aspects of care, however outcome typically refers to:
- A . Health status-related indicators such as whether the pain subsided
- B . Desired results
- C . Appropriate and potentially harmless care
- D . Special set of clinical activities
Knowledge about _______ is crucial to making valid judgments about quality of care using either
process or outcome measures. If we know that a given clinical intervention was undertaken in circumstances that match those, under which the intervention has been shown to be efficacious, we can be confident, that the care was appropriate and, to the extent of good quality.
- A . Outcomes
- B . Structure
- C . Efficacy
- D . Processes
Universities often evaluate applicants for admission on the basis of, among other things, the applicants’ scores on standardized tests. The scores are thus one of the criteria by which program judge the Quality of their applicants. However, although two programs may use the same criterion C scores on a specific standardized examination-to evaluate applicants, the programs may differ markedly on standards: One program may consider applicants acceptable if they have scores above the 50th percentile, whereas the score above the 90th percentile may be the standard of acceptability for the other program.
This example clearly defines the difference between:
- A . Sources and structure
- B . Criteria and standards
- C . Processes and outcomes
- D . Efficacy and equity
For cheing the outcomes our focus of attention is blood pressure of patients with diabetes.
Its criteria and standard can be respectively:
- A . Criterion: Percentage of post heart atta patients prescribed beta-bloers on discharge and Standard: At least 96% of heart atta patients receive a beta-bloer prescription on discharge
- B . Criterion: Percentage of patients with diabetes whose blood pressure is at or below 130/85 and Standard: At least 50% of patients with diabetes have blood pressure at or below 130/85
- C . Criterion: Sugar level in blood on daily basis and Standard: How many times sugar level rises and how many times it declines in a week
- D . None of these
When formulating medical standards, a critical decision that must be made is the _____ at which the standard should be set.
- A . Depth
- B . Clarity
- C . Level
- D . utility of measurement
_________________ standards denote level of quality that can be reached under the best conditions, typically conditions similar to those under which efficacy is determined. These standards are especially useful as a reference points being evaluated should set as a benchmark.
- A . Optimal standards
- B . Minimal standards
- C . Achievable standards
- D . Something in between
___________________ is a difference between an observed event and a standard or norm. Without this standard, or, best practice, measurement of variation offers little beyond a description of the observations.
- A . Variation
- B . Process variation
- C . Assignable variation
- D . Random variation
Measurement of variation in health care and its application to quality improvement must begin with the identification and articulation of:
- A . What is to be measured?
- B . Assignable variation
- C . The standard against which is to be compared a process based on extensive research, trial and error and collaborative discussion
- D . Understanding true variation versus artifact or statistical error
__________________ arises from a single or small set of causes that are not part of event or process and therefore can be traced, identified and implemented or eliminated. In general, researchers are interested in this variation because they can link-or-assign variation to a single specific cause and act accordingly.
- A . Process variation
- B . Assignable variation
- C . Random variation
- D . Performance variation
He used his understanding of statistics to design tools to respond to variation. Following his arrival at Western Electric Co. in 1924, Shewhart introduced the concepts of common cause, special cause variation and statistical control. He designed these concepts to assist Bell Telephone of repairs within its transmission systems.
Who is he?
- A . W. Edwards Deming
- B . Josph M. Juran
- C . Walter Shewhart
- D . Armand Shewhart
In the 1970s, Deming developed his 14 points for western Management in response to requests from U.S. managers for the secret to the radical improvement that Japanese companies were achieving in a number of industries. As part of his “system of profound knowledge,” Deming promoted that “around 15% of poor quality was because of workers, and the rest of 85% was due to bad management, improper systems and processes.” The “system” is based on parts.
Which o the following is/are NOT out of those parts?
- A . Appreciation for a system
- B . Knowledge about variation
- C . Theory of knowledge
- D . Sociology
Joseph juran defined quality as consisting of two different but related concepts. The first form of quality is income oriented and includes features of t he product t hat meet customer needs and thereby produce income (i.e., higher quality costs more).
The second form of quality is cost oriented and emphasizes:
- A . Freedom from failures
- B . Freedom from deficiencies
- C . Knowledge abut variation
- D . Both A and B
Juran Trilogy includes all the following sub-points under the major heading of quality planning EXCEPT:
- A . Identify who the customers are
- B . Determine the needs of those customers
- C . Develop a process that is able to produce the product
- D . Optimize the product feature to meet our needs and customer needs
Overproduction
Inventory
Repairs/rejects
Motion
Processing
Waiting
Transport
These are the types of _____________ identified by Taiichiohno.
- A . Waste (activities that do not add value to the process)
- B . Continuous improvement
- C . Quality controls
- D . Areas to be focused during production
TQC is excellence driven rather than defect driven-a system that integrates:
- A . Quality development, quality improvement and quality maintenance
- B . Quality improvement and quality maintenance
- C . Quality development, quality improvement and quality assessment
- D . Quality improvement and quality maintenance
Crossby’s quality improvement process is based on the Absolutes of Quality Management.
Which of the following is/are out of those absolutes?
- A . Quality is defined as conformance to requirements, not as goodness or elegance
- B . The system for causing quality is prevention, not appraisal
- C . The performance standard must be zero defects, not “that’s close enough”
- D . All of the above
Quality improvement approaches are derivatives and models of the ideas and theories developed by thought leaders and include all of the following EXCEPT:
- A . PDCA/PDSA
- B . ISO 2001
- C . Baldrige criteria
- D . Associate for process improvements
The following diagram shows:
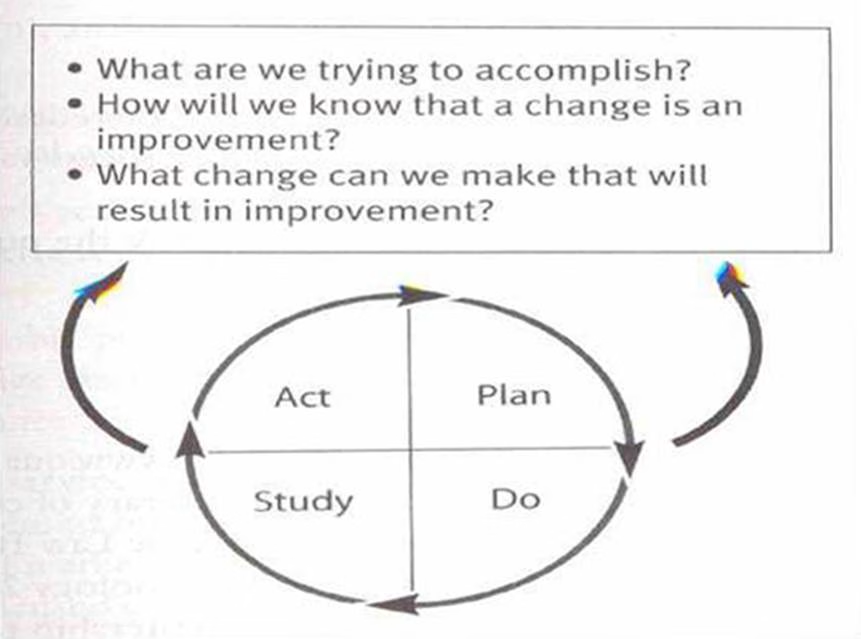

- A . Baldrige criteria for improvement
- B . API Improvement model
- C . Quality improvement
- D . None of these
The Baldrige criteria were originally developed and applied to business; however, in 1997, healthcare-specific criteria were created to help healthcare organizations address challenges such as focusing on core competencies, introducing new technologies, reducing costs, communicating and sharing information electronically new alliance with healthcare providers, and maintaining market advantage. The Baldrige healthcare criteria are built on the set of interrelated core values and concepts.
Which of the following is NOT out of those values and concepts?
- A . Focus on the present
- B . Valuing of staff and partners
- C . Agility
- D . Visionary leadership
Baldrige’s scoring system is based on a __________point scale. Each of seven criteria is assigned maximum value ranging from 85 to 450 maximum points.
- A . 500 points
- B . 1000 point scale
- C . 2000 point scale
- D . 1500 point scale
The weight of scoring system is based on an emphasis Baldrige places on ___________ and an organization’s ability to demonstrate performance and improvement in the following areas:
Product and service outcomes
Customer-focused outcomes
Financial and market outcomes
Workforce-focused outcomes
Process effectiveness outcomes
Leadership outcomes
- A . Results
- B . Output
- C . System perspective
- D . Values
The focus of Lean methodology is a “ba to basics” approach that places the needs of customer first through five steps.
Which of the following is NOT out of those steps?
- A . Define value as determined by the customer
- B . Identify the value stream
- C . Make value identifying steps
- D . Let the customer pull the product
Although Lean thinking focuses on removing waste and improving flow, it also has some secondary effects such as:
- A . Quality is improved
- B . Simplification of processes results in less time in process
- C . Reduces the chances of damage
- D . All of these
Six sigma (3.4 defects per million) is a system for improvement developed over time by Hewlett-Paard, Motorola, General Electric, and others in the 1980s and 1990s.
The aim of six sigma is:
- A . To remove bloages in process
- B . To reduce variations (eliminate defects) in processes
- C . To counter the wastage of activities
- D . To control and analyze the related and unrelated activities
By using a set of statistical tools to understand the fluctuation of a process, management can predict the expected outcome of that process. If the outcome is not satisfactory, management can use associated tools to further understand the elements influencing that process. Six sigma includes process steps which are commonly known as ____________.
- A . DAMIC
- B . PDCA
- C . DAMIE
- D . PDSA
One of the difficult things about quality is explaining how _________ is different from a process or system.
- A . Tools
- B . Methods
- C . Control
- D . A and B are same
The American Society for Quality has formed six categories of quality tools.
Which of the following is NOT out of those categories?
- A . Cause Analysis
- B . Evaluation and decision making
- C . Process analysis
- D . Idea adoption
A Japanese tool called 5S (each step starts with letter “S”) is a systematic program that helps workers take control of their workspace so that it actually works for them (and their customers) instead of being a neutral or, as is quite common, competing factor.
Which of the following is/are NOT out of these five 5S?
- A . Seiton
- B . Seiso
- C . Shitsake
- D . Seiku
Within any unit, organization, or system, there will be barriers to spread and adoption (e.g., organizational culture, communication, leadership support).
However, failure to transfer knowledge effectively may result in:
- A . Unnecessary waste
- B . Inconsistency
- C . organizational persistence
- D . Benchmarks
Rapid cycle testing is designed to reduce the cycle time of new process implementation from months to days.
To prevent unnecessary delays in testing or implementation, teams or units using rapid cycle testing must remain focused on the testing of solutions and avoid:
- A . Over-analysis
- B . Multiple PDSA cycles
- C . Buy-in
- D . Focused testing
Organizational size affects the ability to disseminate best practices
- A . True
- B . False
- C . Difficult to decide
- D . It depends on situation
A social service department regularly monitors the number of inappropriate referrals, the timeliness of discharge planning, and the number of days of discharge delays.
What additional monitor should be added to evaluate the appropriateness of social service interventions?
- A . Inadequacy of documentation in progress notes
- B . Attainment of social service goals
- C . Timeliness of referrals to social services
- D . Number of social service referrals from nursing
The primary purpose of a management information system is to:
- A . Provide data for quality assessment.
- B . Computerize operations for greater effectiveness.
- C . Guarantee better coordination of organizational change.
- D . Provide information that facilitates management decisions.
One major difference between traditional quality assurance (QA) and quality improvement (QI) is that QI:
- A . Stresses peer review, while QA focuses on the customer.
- B . Focuses on the individual, while QA focuses on the process.
- C . Stresses management by objective, while QA stresses team management.
- D . Focuses on the process, while QA focuses on individual Performance
Which of the following processes is most cost-effective in preventing unnecessary resource consumption in the hospital?
- A . Effective preadmission screening
- B . Accurate DRG assignment at admission
- C . Second opinions for all surgeries
- D . Preadmission insurance benefit denials
The primary benefit of adopting a countrywide or global uniform set of discharge data is to:
- A . Facilitate computerization of data.
- B . Validate data being collected from other sources.
- C . Facilitate collection of comparable health information.
- D . Assist medical records personnel in collecting internal data.
Which of the following process can be judged as having highest quality of care?
- A . Successful completion of a surgical operation
- B . Successful completion of a surgical operation and a good recovery
- C . Successful completion of a surgical operation, a good recovery and ascertaining that the operation was indicated
- D . Successful completion of a surgical operation, a good recovery and ascertaining that the operation was not indicated
The concept of cost-effectiveness in Healthcare delivery means:
- A . A proportionately justified improvement in health status of patient is obtained comparing to the cost incurred.
- B . Little improvement in Health status of patient is obtained at a very high cost
- C . Little improvement in Health status of patient is obtained at a very low cost
- D . Great improvement in Health status of patient is obtained at a very low cost
Interpersonal relationships are the fundamental part of a management system. They basically coordinate activities of different departments in a unit.
What is the role of Interpersonal relationships in Healthcare delivery systems?
- A . Promotion of cordial relationships
- B . Clinicians who relate well to their patients are more likely to elicit a more complete and accurate
history from their patients - C . It relates to Medical Ethics
- D . None of the above
IHI has designed a model to support its breakthrough collaborative series.
A key component of the collaborative model is the ability of participants to work with other organizations to discuss:
- A . Different problems
- B . Lessons learned
- C . Barriers to improvement
- D . Both B and C
Employees involved in quality circles are encouraged to develop ideas for improvement or request management efforts to propose solutions for adoption.
The aims of the quality circle activities are all of the following EXCEPT:
- A . Contribute to the improvement and development of the enterprise
- B . Respect human relations and build a workshop offering job satisfaction
- C . Deploy human capabilities fully and draw out infinite potential
- D . Avoid sharing o optional measures
During improvement in healthcare system, because of a combination of technical complexity, system fragmentation, a tradition of autonomy, and hierarchical authority structures, overcoming the “daunting barrier to creating the habits and beliefs of common purpose, teamwork and individual accountability” necessary for spread and sustainability will require:
- A . Continual focus
- B . Commitment
- C . Focus to maintain benchmark levels
- D . Right time
The increased focus on and mandate for healthcare data place healthcare providers in a different situation than they have known in the past. Providers document such things and, unfortunately, many providers struggle to address the measurement mandate proactively, which leads organizations to assume a defensive posture when external organizations release the data.
Which of the following ways show/s the responses of provider in such cases?
- A . The data are old (typically one or two years) and do not reflect our current performance
- B . The data are not stratified and do not represent appropriate comparisons.
- C . Our patients are siertan those at the other hospitals in our comparison group (i.e., no risk adjustments were made to the data).
- D . We can move in a better way without doing competition with others
A more proactive posture would be to develop an organization-wide approach to quality measurement that meets both internal and external demands.
This approach is:
- A . A task that should be completed at once
- B . A task that should be done in chunks of improvement process
- C . Not a task that can be completed once, rather a journey that has many potential pitfalls and detours
- D . A task that should be completed through a series of related activities
This example shows the relationship between:
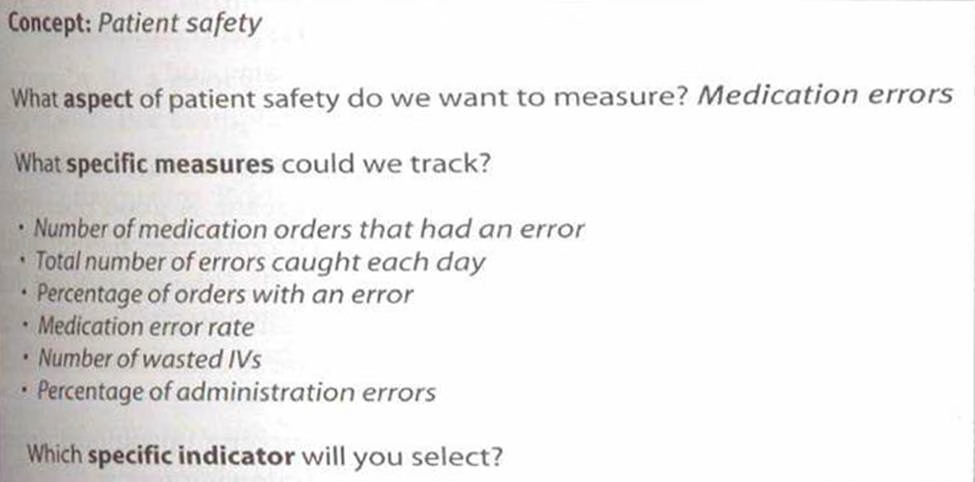

- A . A concept and specific measures
- B . Specific indicator and milestone
- C . Specific measures and specific indicators
- D . Effectiveness and concept
In healthcare, many terms call for more precise operational definitions that how do an organization define the terms such as:
- A . Qui turnaround time
- B . An accurate environmental compliance
- C . A patient fall (a partial fall, a fall with injuries, or an assisted fall)
- D . Surgical end time
Stratification is the separation and classification of data into reasonably homogenous categories. It allows understanding of differences in the data caused by all of the following EXCEPT:
- A . Day of the week
- B . Time of the day
- C . Type of order
- D . Area of facility
“A quality improvement team is interested in determining the percentage of medication orders that are delivered to nurses’ stations within one hour of the order’s receipt in the pharmacy. Before collecting data on this question, the team should determine whether it believes that this percentage could differ by floor, time of day, day of week, type of medication ordered, pharmacist on duty, or volume of orders received. If the team believes that one or more of these factors will influence the outcome, it should take steps to ensure that it collects the data relevant to these factors each time the pharmacy receives an order.”
This example explains:
- A . How stratification could be applied to pharmacy
- B . Is there any need to sample the data
- C . Targets and goals of measurement
- D . Confidentiality issues in measurement
Sampling is a key that healthcare professionals need to develop. If a process does not generate a lot of data, you probably will analyze all the occurrences of an event and not need to consider sampling.
Sampling usually is not required when the measure is:
- A . A percentage
- B . A rate
- C . A step by step process
- D . A strata
_______________ is based on a simple principle-statistical probability. In other words, within a known population of size n, there will be a fixed probability of selecting any single element.
- A . Probability sampling
- B . Random sampling
- C . Systematic sampling
- D . Non-probability sampling
If you decided to interview ten patients in your emergency room on a given day and drew conclusions about your emergency services from these people. You have taken limited data and made a huge jump in logic.
This jump is known as:
- A . Stereotyping
- B . Over-generalization
- C . Ecological fallacy
- D . Quota sampling
Quality circles are groups of five to ten employees, with management support, who meet to solve problems and implement new procedures.
The aim/s of quality circle activities is/are:
- A . Contribute to implement and development of the enterprise
- B . Respect human relations and build a workshop offering job satisfaction
- C . Deploy human capabilities fully and draw out finite potential
- D . Both A and B
Basically an operational definition is a description in quantifiable terms, of what to measure and the specific steps needed to measure it constantly.
A good operational definition:
- A . Gives communicable meaning to a concept or an idea
- B . Is no doubt clear but somewhat ambiguous
- C . Is a decision-making criteria
- D . Enables consistently in data collection
Using the same operational definition becomes even more critical if you are trying to compare several hospitals or clinics in a system. When national hospitals are made, the operational definition challenge becomes extremely complex. All good measurements begin and end with_____________.
- A . An objective and an outcome respectively
- B . A vision
- C . An operational definition
- D . A milestone
The problem with using readily available, convenient data is that the data usually do a poor job of answering the questions necessary to access performance. Ten years ago this “good enough” approach to data collection might have been acceptable. Today, however, because of the increasing demand to demonstrate effectiveness of care and efficiency of healthcare processes, this mind set is not acceptable. Performance quality and excellence do not occur because organizations do what they have always done or what is convenient.
Most healthcare observers agree that:
- A . Specific measures should not be used in data collection
- B . Industry does not need perpetuation of status quo
- C . Quality improvement efforts definitely end up with a positive result
- D . Once you have resolved the issues, the data collection should go smoothly
The data collection phase of the journey consists of two parts: (1) Planning for data collection and (2) The actual data gathering. A well designed data collection strategy should address different analytical questions.
Which of the following is/are the part of planning section for data collection?
- A . Will the data add value to your quality improvement efforts?
- B . How often and for how long will you collect the data?
- C . Will collecting these data have negative effects on patients or employees?
- D . Do you have target and goals for the measures?
Once you have resolved these issues, the data collection should go smoothly. Unfortunately, many quality improvement teams do not spend sufficient time discussing their data collection plans. They want to move immediately to data collection step.
This haste usually guarantees that the team will:
- A . Reschedule the time and cost
- B . Collect too much (or too little) data
- C . Collect the wrong data
- D . Become frustrated with the entire measurement journey
Two key data collection skills satisfaction and sampling enhance any data collection effort. These skills are based more on___________ and _____________ then on statistics, yet many healthcare professionals have received limited training in both concepts.
- A . Logic and reliability
- B . Relatedness and latest happenings
- C . Ethics and reliability
- D . Logic and clear thinking
Stratification is the separation and classification of data into reasonably homogenous categories, within the data, that are mutually exclusive and facilitate:
- A . Data collection efforts
- B . Discovery of patterns that would not be observed id data were aggregated
- C . Skills that are based more experience than knowledge
- D . frustrated measurement process
For example, if you are using a survey to gather patient satisfaction feedback by email, you would not send a survey t o ever y patient. You would start by sending surveys t o roughly 50 percent of the patients an see how many are returned. This limited survey allows you to determine the response rate. Assume that 25 percent of these patients return the surveys. The next task is to determine how representative of the total population these respondents are. To test this question, you need to develop a profile of the total population. Typically, this profile is based on standard demographics such as gender, age, type of visit, payer class, and whether the respondent is a new or returning patient. If the distribution of these characteristics in the sample is similar (within 5 percent) to that found in the total population, you can be comfort able t hat your sample is reasonably representative of the population. If the characteristics of the sample and the population show considerable variation, however, you should adjust your sampling plan. This example clarifies that:
- A . A well-drawn sample, therefore, should be representative of the larger population
- B . The basic purpose of sampling is to be able to draw a limited number of observations
- C . Sampling is probably the most important thing you can do to reduce the amount of time and
resources spent on data collection - D . Sampling consists of series of compromises and tradeoffs
All of the following are characteristics of probability sampling EXCEPT:
- A . A specific statistical design is followed
- B . The selection of items from the population is determined solely according to known probabilities by means of a random mechanism, usually using a table of random digits
- C . The sampling error (i.e., the difference between results obtained from a sampling survey and results that would have been obtained from a census of the entire population conducted using the same procedure as in sampling survey) can be estimated, and, as a result, the precision of the sample result can be evaluated.
- D . Listing of selected sample on a priority basis on a sampling sheet
Systematic sampling is achieved by numbering or ordering each element in the population (e.g., time order, alphabetical order, and medical order) and then selecting every kth element.
The key point that most people ignore when doing a systematic sample is that:
- A . The starting point for selecting every kth element should be guaranteed through a random process and should be equal to or less than k but greater than zero.
- B . The starting point for selecting every kth element should be guaranteed through a random process and should be less than k but greater than zero.
- C . The starting point for selecting every kth element should be guaranteed through a random process and should be greater than zero.
- D . The starting point for selecting every kth element should be guaranteed through a random process and should be equal to or greater than zero.
A random sampling also can be drawn by placing equally sized pieces of paper with a range of numbers on them (e.g., 1 to 100) in a bowl and picking a predetermined number to be the sample.
The problem with simple random samples is that:
- A . They may under represent segments of population
- B . They may over represent segments of population
- C . They may over or under-represent segments of population
- D . They cannot truly depict the samples
Convenience sampling produces a biased sample that is basically a collection of anecdotes that cannot be applied generally to larger populations.
Convenience sampling is also known as:
- A . Quota sampling
- B . Judgment sampling
- C . Expert sampling
- D . Chunk sampling
Quota sampling was developed in the late 1930s and used extensively by the Gallup organization. Babbie (1979) describes the steps involved in developing a quota sample.
All of the following are out of those steps EXCEPT:
- A . Develop a matrix describing the characteristics of the target population. This may entail knowing the proportion of male and female; various age, racial and ethnic proportions; as well as the education and income levels of the population
- B . Once the matrix has been created and a relative proportion assigned to each cell in the matrix, data are collected from persons having all the characteristics of a given cell
- C . All persons in a given cell are then assigned a weight appropriate to their proportion of the total
- D . When all the sample elements are so weighted, the overall data should provide a reasonable representation of the majority of the samples
Statistical analysis conducted with control charts is different from what some consider “traditional research” (e.g. hypothesis testing, development of p-values, design of randomized clinic trials). Traditional research is designed to compare the results at time one (e.g. the cholesterol levels of a group of middle-aged men) with the results at time two (typically months after the initial measure). Research conducted in this manner is referred to as___________________.
- A . Static group comparison
- B . Continuous distribution
- C . SPC
- D . None of these
When groups are asked to evaluate how effective they are with respect to will, ideas and execution, they consistently provide bothersome answers. Self-assessment to hundreds of healthcare professional is administered in United States and abroad.
Most respondents mark:
- A . High for will, medium to high for ideas and high for execution
- B . Low for will, medium to high for ideas and low for execution
- C . High for will, medium to high for ideas and low for execution
- D . High for will, medium to high for ideas and low for execution
Which of the following is NOT out of Quality measurement categories or domains?
- A . Clinical quality (including both process and outcome measures)
- B . Financial performance
- C . Operational status
- D . patient satisfaction
Generally, medical record review and prospective data collection are considered the most time-intensive and expensive ways to collect information.
Many reserve these methods for highly specialized improvement projects or use them to answer questions that have:
- A . Surfaced following review of administrative data sets
- B . Use rule-based software development
- C . Combine code and chart based on the overall population
- D . Situation related characteristics
A data analyst, using a clinical decision support system (administrative database), discovered a higher-than-expected incidence of renal failure (a serious complication) following coronary artery bypass surgery. The rat e was well above 10 percent for the most recent 12 months increased over the last six quarters. However, the clinical decision support system did not contain enough detail to explain whether this complication resulted from the coronary artery bypass graft procedures or was a chronic condition present on admission.
To find the answer, the data analyst use different steps.
This example illustrates:
- A . How an administrative system’s cost effectiveness can be combined with the detailed information in a medical record review?
- B . How data analyst use review chart to isolate cases
- C . That data should be thorough
- D . Computer aided information systems are better to gather data
The syndrome of stockpiling is proven to be ineffective and inefficient. It also creates quality issues. This approach provides little value to the data collection effort and is one of the biggest mistake quality improvement teams make.
Rather than provide a rich source of information, this approach unnecessarily derives up:
- A . The cost of data collection
- B . Create data management issues
- C . Overwhelms the quality improvement teams with too much information
- D . All of the above
The distinction between inpatient and outpatient data is an important consideration in planning the data collection process because:
- A . The data sources may be different
- B . Mixing of data may or may not be reliable
- C . Approaches to data collection may be different
- D . Both A & B
What approach should be followed by the healthcare improvement team for the best outcomes?
- A . Data collection should be thorough. The team may need the data down the road
- B . Stockpiling of data “just in case”
- C . Collecting the critical few rather than collecting for a rainy day
- D . Collection of a balanced amount of data in order to full-fill the current demands
To identify outpatient data sources, the team should consider the following questions EXCEPT:
- A . Are the physician in organized medical groups that have outpatient electronic medical records, which could be a source of data? Will their financial or billing systems be able to identify all patients with diabetes in their practices?
If not, can the health plans in the area supply the data by practice site or individual physician? - B . Some of the most important diabetes measures are based on laboratory testing. Do the physicians have their own labs? If so, do they achieve the laboratory data for12-24 month snapshot? If they do not do their own lab testing, do they use a common reference lab that would be able to supply the data?
- C . Do the measures selected by team reflect the aspects of care that have the most influence on patient’s outcome
- D . Do the source outpatient data is the same as inpatient data
Which of following objectives is/are NOT essential for successful quality improvement project and data collection initiative?
- A . Identify the purpose of the data measurement activity (for monitoring at regular intervals, investigation over a limited period, or one time study).
- B . Identify the most appropriate data sources
- C . Identify the most important measures for collection (the critical few).
- D . Commonsense all the data collected that will provide the actual information
Some database projects rely on medical record review because many of the data are not available in administrative database, e.g.
- A . Measurement that require time stamp, such as administration of antibiotics within one hour before surgical incision
- B . Patient’s entries and visits to the physician
- C . Patient’s of test and lab reports
- D . Nursing record