MRCPUK SEND Endocrinology and Diabetes (Specialty Certificate Examination) Online Training
MRCPUK SEND Online Training
The questions for SEND were last updated at Dec 19,2025.
- Exam Code: SEND
- Exam Name: Endocrinology and Diabetes (Specialty Certificate Examination)
- Certification Provider: MRCPUK
- Latest update: Dec 19,2025
30-532
Results from an MR scan of pituitary are shown (see image).
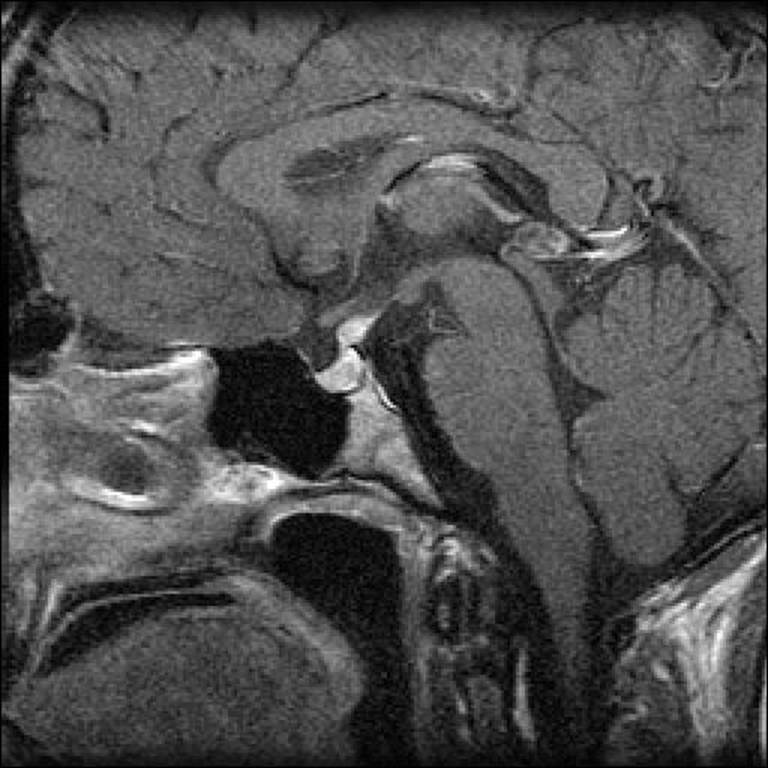
What is the most likely diagnosis?
- A . autoimmune (lymphocytic) hypophysitis
- B . craniopharyngioma
- C . non-functioning pituitary adenoma
- D . psychogenic polydipsia
- E . Rathke’s cleft cyst
A 52-year-old man had been found to have type 1 diabetes mellitus at the age of 25. He had developed retinopathy at the age of 31 and a painless foot ulcer at the age of 40. His renal function had subsequently deteriorated.
On examination, urinalysis showed protein 1+, glucose 2+.
What is the most likely diagnosis?
- A . focal segmental glomerulosclerosis
- B . membranoproliferative glomerulonephritis
- C . minimal change glomerulonephritis
- D . nodular glomerulosclerosis
- E . tubulointerstitial nephritis
A 19-year-old man was seen in the diabetes clinic. He had lost 2 kg in weight since the diagnosis of diabetes mellitus 18 months previously. At presentation, his body mass index was 33 kg/m2 (18C25), his random plasma glucose was 18.0 mmol/L and his haemoglobin A1c was 56 mmol/mol (20C42). He was taking gliclazide, and metformin had been added later. His father and grandfather had developed diabetes mellitus during their twenties.
Investigations:
haemoglobin A1c56 mmol/mol (20C42)
serum C-peptide301 pmol/L (180C360)
anti-glutamic acid decarboxylase (GAD)
antibodiesnegative
What is the most likely diagnosis?
- A . chronic pancreatitis
- B . latent-onset diabetes of autoimmunity
- C . maturity-onset diabetes of the young
- D . type 1 diabetes mellitus
- E . type 2 diabetes mellitus
A 46-year-old South Asian man presented with a 2-month history of dry mouth and polyuria. He had hypertension treated with bendroflumethiazide. There was no family history of diabetes mellitus, but his father had died suddenly during lower limb angioplasty at the age of 51.
On examination, the patient’s pulse was 76 beats per minute and regular, and his blood pressure was 164/86 mmHg. The rest of the physical examination was normal. Urinalysis was normal.
Investigations:
serum sodium143 mmol/L (137C144)
serum potassium3.0 mmol/L (3.5C4.9)
serum creatinine123 µmol/L (60C110)
fasting plasma glucose6.9 mmol/L (3.0C6.0)
What is the most appropriate next step in management?
- A . change bendroflumethiazide to ramipril
- B . haemoglobin A1c measurement
- C . oral glucose tolerance test
- D . repeat fasting plasma glucose
- E . start oral hypoglycaemic treatment
A 35-year-old woman was referred with a left lower thyroid lesion. She was asymptomatic.
Examination confirmed the presence of a 2 ? 3-cm, firm, mobile, non-tender mass.
Investigations:
ultrasound-guided fine-needle aspiration biopsyThy 5
How is Thy 5 defined?
- A . abnormal, diagnostic of malignancy
- B . abnormal, suspicious (but not diagnostic of) malignancy
- C . follicular lesions
- D . non-diagnostic or inadequate
- E . non-neoplastic (consistent with nodular goitre or thyroiditis)
A 55-year-old woman presented complaining of difficulty losing weight.
On examination, her blood pressure was 170/105 mmHg and urinalysis showed protein 1+.
An ultrasound scan of abdomen revealed a 4.5-cm solid lesion in the right adrenal gland.
She was treated with ramipril and further endocrine evaluation was performed.
Investigations:
serum potassium3.6 mmol/L (3.5C4.9)
serum creatinine135 µmol/L (60C110)
plasma renin activity:
(after 30 min supine)3.9 pmol/mL/h (1.1C2.7)
(after 30 min upright)6.8 pmol/mL/h (3.0C4.3)
plasma aldosterone:
(after 30 min supine)150 pmol/L (135C400)
(after 4 h upright)350 pmol/L (330C830)
serum cortisol (09.00 h)650 nmol/L (200C700)
serum cortisol (22.00 h)225 nmol/L (50C250)
24-h urinary free cortisol230 nmol (55C250)
24-h urinary dopamine3200 nmol (<3100)
24-h urinary adrenaline120 nmol (<144)
24-h urinary noradrenaline450 nmol (<570)
What is the most appropriate initial management of the adrenal lesion?
- A . ?-adrenoceptor blockade
- B . angiotensin-2 receptor blockade
- C . medical observation with annual ultrasonography
- D . mineralocorticoid receptor blockade
- E . surgical excision
A 26-year-old woman was referred by her general practitioner for the management of subfertility. Her menarche had occurred at the age of 14 and she had experienced oligomenorrhoea since the age of 16. She also complained of gradually worsening hirsutism since puberty.
Clinical examination showed central obesity, a body mass index of 32 kg/m2 (18C25) and a blood pressure of 140/90 mmHg.
The following results were obtained within 1 week of her last menstrual period.
Investigations:
overnight dexamethasone suppression test (after 1 mg dexamethasone):
serum cortisol30 nmol/L (<50)
serum dehydroepiandrosterone sulphate12 µmol/L (3C12)
serum androstenedione10.0 nmol/L (0.6C8.8)
serum 17-hydroxyprogesterone38 nmol/L (1C10)
serum oestradiol200 pmol/L (200C400)
serum testosterone3.5 nmol/L (0.5C3.0)
serum sex hormone binding globulin30 nmol/L (40C137)
plasma follicle-stimulating hormone4.0 U/L (2.5C10.0)
plasma luteinising hormone6.0 U/L (2.5C10.0)
What is the most likely diagnosis?
- A . adrenal androgen-secreting tumour
- B . Cushing’s syndrome
- C . late-onset congenital adrenal hyperplasia
- D . ovarian androgen-secreting tumour
- E . polycystic ovary syndrome
A 16-year-old boy was referred to the endocrine clinic with symptoms of delayed puberty.
On examination, he had a reduced sense of smell, small-sized testes and underdeveloped secondary sexual characteristics.
Investigations:
serum testosterone3.5 nmol/L (9.0C35.0)
serum follicle-stimulating hormone1.0 U/L (1.0C7.0)
serum luteinising hormone1.5 U/L (1.0C10.0)
serum prolactin220 mU/L (<360)
MR scan of brainnormal
He asked about his future fertility.
What will be the most useful agent for him to achieve fertility?
- A . bromocriptine
- B . clomifene
- C . gonadotropin-releasing hormones
- D . octreotide
- E . testosterone
A 32-year-old man presented to the emergency department after becoming acutely unwell.
He had a 5-year history of type 1 diabetes mellitus and no other significant medical history.
On examination, he was apyrexial, his pulse was 120 beats per minute, his blood pressure was 96/58 mmHg and his respiratory rate was 32 breaths per minute.
Investigations:
random plasma glucose14.2 mmol/L
arterial blood gases, breathing 60% oxygen:
PO28.9 kPa (11.3C12.6)
PCO22.6 kPa (4.7C6.0)
pH7.10 (7.35C7.45)
H+79 nmol/L (35C45)
bicarbonate6.1 mmol/L (21C29)
base excessC18 mmol/L (±2)
What diagnosis is most likely to account for these results?
- A . acute asthma
- B . acute myocardial infarction
- C . diabetic ketoacidosis
- D . diabetic ketoacidosis and pulmonary embolism
- E . salicylate poisoning
An 80-year-old man was referred because of weight gain and low mood but said he was otherwise well. He had a complex cardiac history including a ventricular fibrillation arrest and a permanent pacemaker, but he had been very well for the past 3 years. He was taking amiodarone 100 mg daily, lisinopril 40 mg daily and furosemide 80 mg daily.
On examination, he had a pacemaker in situ and his pulse was 84 beats per minute and regular. He had a 2/6 mid-systolic murmur in the aortic area with no radiation, mild ankle oedema, and scanty basal crackles bilaterally on auscultation of his chest.
Investigations (before attending clinic):
serum thyroid-stimulating hormone19.0 mU/L (0.4C5.0)
serum free T411.0 pmol/L (10.0C22.0)
anti-thyroid peroxidase antibodies300 IU/mL (<50)
What is the most appropriate next step in management?
- A . review with repeat thyroid tests in 3 months
- B . start levothyroxine 25 micrograms daily
- C . start levothyroxine 100 micrograms daily
- D . start liothyronine sodium 10 micrograms twice daily
- E . stop amiodarone
Latest SEND Dumps Valid Version with 200 Q&As
Latest And Valid Q&A | Instant Download | Once Fail, Full Refund
